
SLEEP STUDY: Robin Silbergleid Investigates Why Her Child Just Won’t Stay Sound and Down
Here is the thing I hope to god my children don’t remember: me, hands shaking, shoving my son’s stroller back and forth over the hump in the kitchen floor and around the living room, furious uncountable laps. I said if he didn’t sleep I would kill him. Part of me meant it.
I literally wasn’t seeing straight—the room around me all waves and curves, a flashing light in the corner of my eye. The baby, ten months, always a horrid sleeper, had been waking every forty minutes all night long for more than a week. When he did sleep, it was with my breast in his mouth. I weighed maybe 95 pounds.
My daughter, eight, sat on the couch, out of the way of my laps, cried, “I can help, I can help.”
Her voice broke me. I sat on the floor with both of them in my arms and sobbed. I made potatoes for lunch. I left the baby with her and a basket of toys, shut myself in the bedroom, and called my mom.

“Hazy” by Andy Kiel / Flickr Creative Commons License
Flash forward three years: We are sitting in the lobby of the University of Michigan “Med Inn.” It is fun right now, the two of us on a trip at a hotel without his sister. There is a bridge from the parking garage to the hospital building, an elevator with buttons to push. He anticipates stickers, attention. I have explained to him that the doctor is going to see why it is that he’s having so much trouble staying asleep at night. We eat our submarine sandwiches and potato chips on a bench outside while the few doctors and nurses who haven’t left for the day—it is now about 6:45 pm—smile as they walk past.
When we are finished with dinner, we take the elevator up to the sleep study waiting room. As I deal with check-in, the signing of many forms, he climbs over from chair to chair.
It’s going to be a long night.
After they call us back to his room, which looks like a cross between a standard hospital room and a cheap motel with a foldout couch/bed for me, it is about a thirty-minute process of two techs hooking him up to electrodes with a paste that sticks to his hair like taffy. They snake wires up from his legs. They wrap the electrodes with gauze as if he’s suffered massive head trauma, and then put a cotton sock like a ski mask on his face to keep everything in place. This includes a “mustache” nasal cannula and a little flap that will tell if he breathes through his mouth instead of his nose. He smiles for the camera when I take his picture but by now the fun has worn off.
I’m just grateful that whatever this study turns up, or doesn’t, my family’s sleep needs are finally being taken seriously.
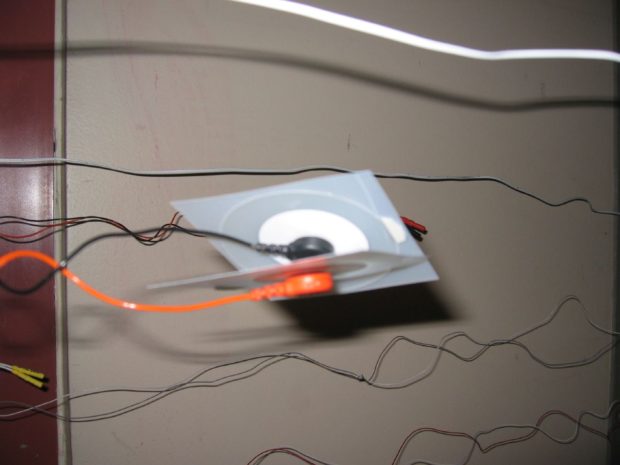
Sensor (sideways) by Russ / Flickr Creative Commons License
After that unfathomable weekend during his infancy, my mother came to rescue us. She slept upstairs with my son. I moved onto the blowup mattress in the dining room. I still heard every squawk, every creak of the floorboards. My breasts filled with milk. She brought him to me every two hours to nurse and, doped up on a combination of Benadryl and wine, I slept more than I had since his birth.
When she left and I could think again, I tried doing research on sleep habits of infants who had been growth restricted, as he was, in utero. I asked my son’s pediatrician about melatonin, about a sleep study. Too young, she said; unnecessary; you just need to fight the battle and let him cry; it might take a while, he’s a stubborn one. She insisted that his problem was “behavioral,” though I’d already raised one child who slept moderately well from infancy on. She put him on the antacid Prilosec for reflux; he woke every two hours instead of every forty minutes.
I went to the internal medicine clinic for a prescription for sleep medication for myself. The young resident gave me a depression inventory and diagnosed me with mild insomnia. I hadn’t slept more than two hours straight in ten months. I wondered what major insomnia would feel like and tried very hard not to laugh in his face.
“Melatonin” by troy / Flickr Creative Commons License
I do not need to cite all the literature that clarifies just how vital sleep is for both mental and physical health. That sleep deprivation is actually a form of torture. That the effects of even short-term sleep loss can be debilitating. What of month after month? I started thinking about how babies end up in microwaves, left on doorsteps, in dumpsters. I started worrying about what starting to think about such tragedies meant.

“sleep bird” by Andrew Smith / Flickr Creative Commons License
Months pass. We have good days. We take walks to the park, to the farmer’s market downtown. We buy vegetables. I make hummus, blueberry muffins. We go to the library, read stories. But as bedtime nears I am full of dread. Even rage.
Months pass. I try many things, I read many books and articles and list servs. White noise. Swaddling. Co-sleeping. He sleeps in my arms in the rocking chair. He sleeps in the crib across from my bed. He sleeps on top of my chest. He cries. Whines. Learns to call “mama.” I move the crib into his own room, so he can’t see me in the dark. I let him cry, some. It just makes the situation worse. He screams for forty minutes, falls asleep, wakes up forty minutes later. I move downstairs so I can’t hear him cry. I’d need to leave the house not to hear him cry.
Months pass. I take my son to the pediatrician. I ask again about melatonin, a sleep study. We have the same conversation at each well-visit. How many times a night does he wake? It depends, I say, two, three, four times. Often, hourly after 3:00 am. What does he want, they ask? What he wants, I insist, is to sleep. He is exhausted. Their answer is always “let him cry.” What I want is for him not to wake. This is a fundamental distinction they do not seem to understand. Their solution is behavior modification. My question is biology. How can letting a child scream for hours in the middle of the night, scream until he throws up or collapses in exhaustion only to wake up thirty minutes later, be an actual strategy for improving sleep? This isn’t a rhetorical question.
The first time my son sleeps an eight hour stretch it is the night of his second birthday; I wake every few hours, panicked that he’s stopped breathing. It never happens again.
*
These days my whole world revolves around sleep. How much he gets, how much I get, which medications to take. I say no to evening events because I need to tuck him in, because I need time to wind down myself. I tell my mother that no we will not be coming home for the holiday weekend unless I am well rested; I will not risk falling asleep behind the wheel, which, ironically, is about the only time I feel myself slipping into sleep on my own. There have been times I have posted a note on my door alerting my daughter: bad night, do not wake us, in the event that she happens to get up before us, the mornings that I have finally fallen back to sleep at 5:00 am after hours of rolling, mornings I don’t care how late we are for daycare and school if it means we can get a few more minutes please, yes please, of sleep.

“Sleepless” by Mimmi Thorneus / Flickr Creative Commons License
As a chronically sleep-deprived single mother of a chronically sleep-deprived child, I find the language many other parents use to talk about sleep habits of “good sleepers” disturbing and dogmatic, incapable or unwilling to understand the nuances of biological and familial factors that go into sleep. If, for example, a mother has successfully used strategies involving ‘crying it out’ or ‘sleep training’ or ‘ferberizing,’ she will tell you that your insomniac child has not learned to ‘self-soothe.’ I have come to loathe the word, which sounds on the surface delightful, something everyone would benefit from. But let me be frank: it is not biologically possible “train” a child to sleep. To be sure, you can use methods to teach children, like Pavlov’s dogs, that crying in the middle of the night will not get them what they want, and eventually, some children will indeed roll over and stop calling. On the other side of the sleep debate, so-called attachment philosophy decrees that sleep-training is terrible, that it can lead to permanent psychological damage, that it’s our job to parent our kids in the night, with the same attention as the day, that we should sleep with them, keep them close, make them feel safe, do whatever they need to help them. That, in essence, parents should never sleep more than a few hours, for years, if that’s what it takes to “parent” through the night.
Let me state for the record, if you found a method, any method, that works for you and your family, amen.
But none of these philosophies help me in the middle of the night when it’s only me, who hasn’t slept well in more than three years, and there’s no one else to call, and if I have to hear him cry, even for a few minutes, I don’t sleep, and then my daughter can’t sleep, and then tomorrow morning will be horrible, I know it already at 3:00 am I won’t be able to work, won’t be able to rest, all of it will be wrong.

by masha krasnova-shabaeva / Flickr Creative Commons License
The sleep study I have been requesting for years comes, finally, after months of back and forth with the pediatrician and the clinic to schedule an initial consult with a team of specialists. I feel on some level ridiculous, like it could not possibly be that bad, that I “just” have a kid who sleeps poorly; the problem must be with me, my parenting, my choice to co-sleep with him during infancy or breastfeed through 22 months, something. But after a month of writing down diligently time of bed and wake, recording naps, night-wakings, it is very clear that my son—who is now 3.5 years old— still wakes two to five times per night, mostly three. Sometimes he’s awake for up to two hours in the middle of the night. That all these months of trying anything, everything, didn’t make much difference. And when we do make it to the consult—when we spend more than an hour going over all variations on these questions about sleep habits and what he looks like sleeping, does he hold his neck arched back and does he kick his legs and what does it sound like when he wakes up gasping, does it come from his nose like a snort or more like a sigh—it’s the morning after a bad night… and I just break down and cry. We know how hard it is, the sleep specialists say, and they actually sound sincere.
The sleep specialists are not dismissive or take the situation lightly; they will help him without making me feel like I have failed. Even if they think it, they do not say his problem is “behavioral”; they say instead that there are habits we might want to change, habits that might have resulted from medical issues in the past or in the present, that they will look at the whole picture. They take blood work. Ask me to continue logging his sleep. We plan the sleep study. They make minor suggestions about our night routine, and it all sounds so reasonable I say of course.
“Macro” by Russ / Flickr Creative Commons License
It’s been a few months since the sleep study, and right now, we are muddling through. The “lost days,” days I can’t function because I’ve been awake since 3:00, are fewer and far between. It has indeed been better since we got medical help, since he was diagnosed (thank you!) with very low iron and possible reflux and placed back on Prilosec and massive doses of chewable iron. Although the official report says his sleep study is negative for apneas, his arousal index (as I have learned to call it) is actually on the cusp, and it is notoriously difficult to do a sleep study on a toddler. Sleep, the specialists say, is complicated, it is a whole family issue. And it is this simple recognition, it turns out, that I have been looking for all along. The awareness that blaming a mother for her child’s poor sleep, especially when she herself is sleep-deprived, doesn’t help anyone in the family, and it certainly doesn’t get any of us more sleep.

These days at bedtime I sit in the rocking chair studying my son. He rolls, kicks the wall, talks to himself as lullabies play on endless repeat on his white noise machine. I remind him to close his eyes. Remind him to stop talking. There is no question, he sleeps more soundly, wakes less frequently, and gets more sleep overall now that he’s on this new regimen. Eventually he puts his left hand inside his pajama shirt, settles. Eventually he begins to snore, and I sneak out, join my older child while she makes her lunch, or sit down to read a book. I go to bed early, still, because that way I get a longer stretch before my son’s first waking. Things are better, to be sure, but he still does not “sleep through the night,” and I wonder if he ever will. Although he falls asleep on his own, in his own bed, he often finds his way to mine; it’s still best for him when he’s curled up with me, feet near my face, when he can reach out and touch me. And sometimes, with our bodies like inverted commas, listening to the steady huff of his exhale, I join him in the dark.
About the Author
Related Posts

There’s Nothing to Fix →

Claiming and Curating Infertility: The Editors of a New Anthology Talk Trauma, Healing, and Creating →

When the Kid Gets Sick: Five Stages →

One Response to SLEEP STUDY: Robin Silbergleid Investigates Why Her Child Just Won’t Stay Sound and Down